Cutting out the Middleman: How States Can Save Medicaid Dollars by Firing Pharmacy Benefit Managers
Examining just 46 drugs known to have significant PBM markups, we find that 13 states could save at least $100,000 to $29 million annually by shifting these drugs to fee-for-service payments — savings that come from reducing corporate markups, not from cutting benefits or pharmacy reimbursements.
Hannah Garden-Monheit, Institute for Responsive Government
Tyler Haydell, Fairmark Partners, LLP
Introduction
Medicaid programs are currently under significant pressure from the passage of H.R. 1 (the “One Big Beautiful Bill”), which cuts federal Medicaid spending by an estimated $911 billion over 10 years — billions of dollars per state — and is projected to increase the number of uninsured by 10 million. H.R. 1 also imposes significant administrative burdens on both American families and states, by creating new work and reporting requirements. Faced with these challenges, cash-strapped states are scrambling to reduce costs.
One way certain states can realize cost savings is by removing Pharmacy Benefit Managers — middlemen known as “PBMs” — from their Medicaid pharmacy benefit programs. Examining just 46 drugs known to have significant PBM markups, we find that 13 states could save at least $100,000 to $29 million annually by shifting these drugs to fee-for-service payments — savings that come from reducing corporate markups, not from cutting benefits or pharmacy reimbursements. More comprehensive estimates indicate potential savings from removing PBMs from Medicaid could be substantially larger — in the tens of millions to billions of dollars per state annually.
The Problem
Many states’ Medicaid programs allow Managed Care Organizations (MCOs) to sub-contract with PBMs to administer their prescription drug benefits, including designing their formularies, negotiating drug prices with manufacturers, and determining reimbursement rates for pharmacies. However, the largest PBMs have a documented history of inflating costs, including by marking up drug costs, pocketing the “spread” between what they charge payors and reimburse pharmacies, extracting fees, and negotiating rebates that drive up the list prices on which patient co-pays are generally based. Indeed, earlier this year the Federal Trade Commission (FTC) found that the three largest PBMs — CVS Caremark, Cigna Group’s Express Scripts, and UnitedHealth Group’s Optum Rx, which collectively control about 80% of all U.S. prescriptions — often marked up specialty generic drugs by thousands of percent, and pocketed billions in revenue via these markups and spread pricing.
The Solution
States can save money by “carving out” prescription drug benefits — i.e., by removing pharmacy benefits from Medicaid managed care and instead administering them directly under the state’s fee-for-service (FFS) program. For example, West Virginia became the first state to do so in 2017, and an actuarial evaluation subsequently estimated the state’s actual cost savings as $54 million in a single fiscal year. Other states that have “carved out” prescription drug benefits likewise projected substantial savings, with California estimating savings of $150-$405 million annually, New York estimating savings of $548 million for FY 2025, and North Dakota estimating savings of $17 million annually. Missouri, Tennessee, and Wisconsin have also shifted their Medicaid drug programs to FFS, though we are unaware of public cost-savings estimates.
In 2019, Ohio undertook a different type of reform, contracting with a single PBM to administer Medicaid pharmacy benefits, rather than leaving contracting to MCOs; an actuarial evaluation estimated Ohio’s savings as $140 million over a two-year period — savings that built upon earlier Ohio efforts to end spread pricing that had cost the state $224.8 million in a one-year period alone. Kentucky Medicaid officials reportedly saved about $283 million over two years by switching to a single PBM — a reform likewise undertaken after an audit found that spread pricing had cost the state $123.5 million in a single year. In the absence of wholesale reforms, states can also potentially save costs by auditing their PBMs. For example, a 2017 audit performed for the Louisiana Department of Health identified at least $42 million in excess drug charges.
To help states understand their potential for cost savings, we calculated a rough estimate of how much states could save by eliminating exorbitant markups on the 46 specialty generic drugs previously identified by the FTC as subject to significant markups by the Big 3 PBMs (see Fig. 2). Specifically, we calculate the cost savings from shifting to reimbursing pharmacies at a flat, readily calculable fee for these 46 drugs: namely, the National Average Drug Acquisition Cost (known as “NADAC”), plus a $10 dispensing fee1.
Our calculations should be understood as a conservative estimate of potential savings that states could achieve through PBM reforms, as they reflect only savings from reducing markups on 46 specific drugs — not the much larger potential cost savings from shifting to FFS reimbursement for all drugs. That is, these estimates do not capture other drugs, and nor do they capture any potential additional savings from eliminating fees, spread pricing, or other extractive PBM practices. States that comprehensively “carve out” pharmacy benefits and shift to fee-for-service reimbursement could thus experience significantly greater savings. For example:
- A study by Strategic Directions Rx estimates that from 2017-2023, Virginia Medicaid plans overspent by $10.86 billion on prescription drugs compared to the national average. A report commissioned by the state found
that spread pricing cost the state $29 million over an 18-month period in 2018-2019 — a distinct form of overcharging from the over $29 million in markups on 46 drugs we identify below. - A study commissioned by the State of Utah Department of Health and Human Services estimates the state could save $2.3 million per year by shifting to FFS reimbursement (using an $11.56 dispensing fee).
- A study commissioned by the Kentucky Department for Medicaid Services estimates potential cost savings as nearly $240 million annually.
- A Pennsylvania Auditor General’s report found that spread pricing cost the state over $40 million in 2017 — a distinct form of overcharging from the $13 million in markups on 46 drugs we identify below.
- A study by the Michigan Pharmacists Association found that spread pricing cost the state at least $64 million between 2016-2018 — a distinct form of overcharging from the nearly $9 million in markups on 46 drugs we identify below.
Moreover, while this paper focuses on savings from removing PBMs from Medicaid pharmaceutical benefits, states could save even more by also shifting medical services to FFS reimbursement. By one estimate, states would have saved $34 billion in 2023 had they used FFS reimbursement for Medicaid providers, instead of relying on MCOs — and the federal government would have saved another $43 billion.
The Potential Savings on 46 Specialty Generic Drugs
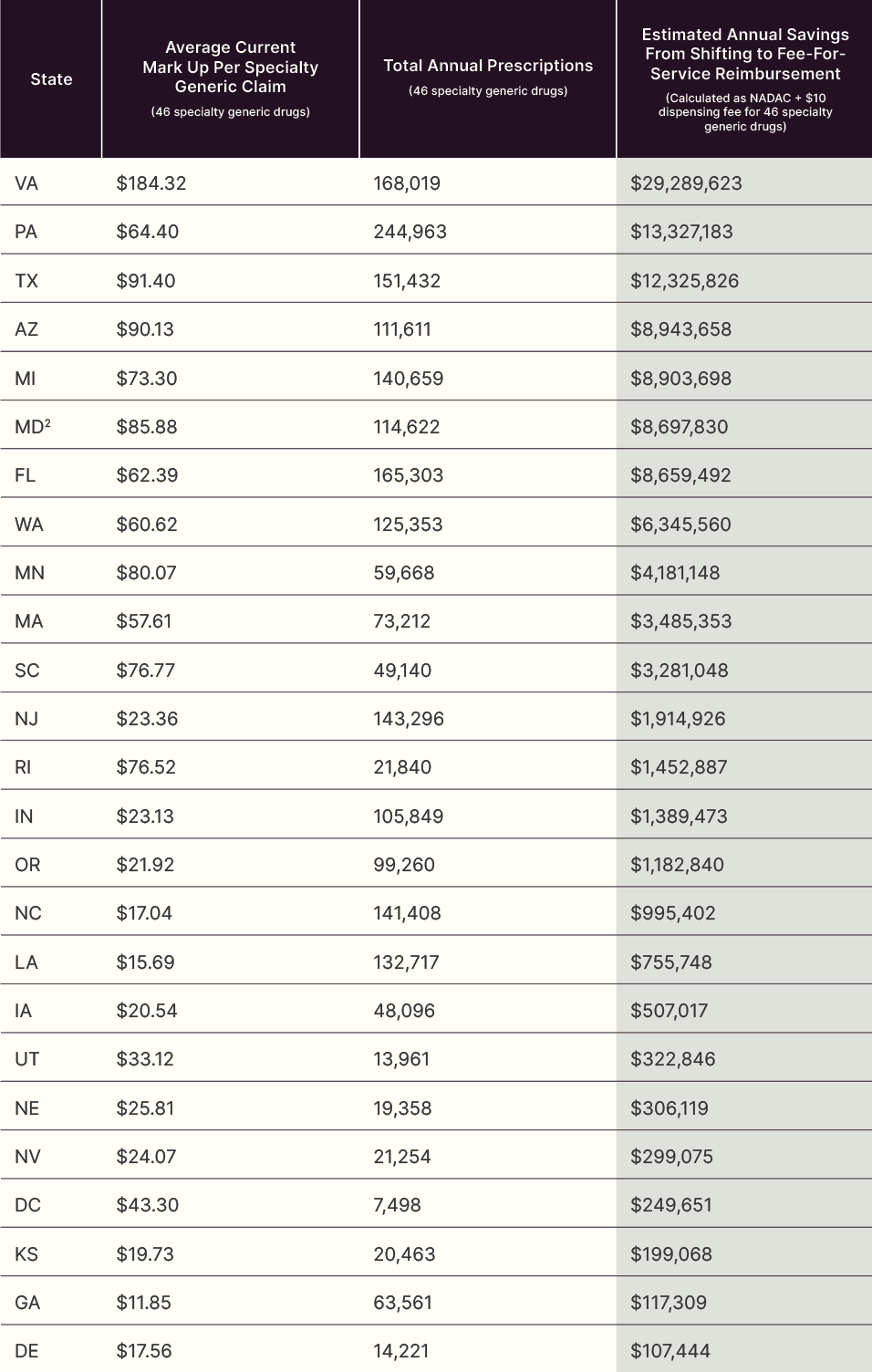
The Medicaid State Drug Utilization Database (SDUD) and National Average Drug Acquisition Cost (NADAC) Database were used for the analysis. Savings are calculated by comparing the amount each state Medicaid plan paid for a drug compared to how much the drug cost to purchase (NADAC), plus a standard dispensing fee of $10. The analysis is limited to the 46 generic specialty drugs identified by the FTC. The analysis covers only states with managed Medicaid programs and excludes fee-for-service Medicaid plans.
To connect with AELP and/or Institute for Responsive Government subject-matter experts on prescription drug supply chains, Medicaid administration, and HR 1 implementation, please contact Hannah@responsivegov.org.
1. A $10 dispensing fee is in line with the dispensing fees currently charged by most states in their FFS programs, per data reported by the Center for Medicaid and CHIP Services.
2. Maryland banned spread pricing in Medicaid in 2020, following a Maryland Department of Health study that found spread pricing by PBMs had cost the state $72 million in 2018. The fact that Maryland’s Medicaid program continues to spend millions annually on markups on these 46 drugs illustrates the need for comprehensive PBM reforms; banning the practice of spread pricing alone is inadequate to stop PBM overcharges.
